
Best Anti-Snoring Device: MAD vs TRD Comparison
The night feels long when someone keeps nudging an elbow into your rib cage. The room goes quiet for a minute or two, and then that rough snore rolls out again.
Morning comes, the clock says eight hours passed, yet both people in the bed feel as if they barely slept at all. This scene is very common.
Snoring does not only mean noise. It can strain relationships, drain energy needed for the coming day, and leave people worried about what is happening.
When someone types “MAD vs. TRD” into a search bar, they are often one of the hardcore sleep-derived legion: tired, frustrated, and overwhelmed by all the gadgets being marketed out there.
Anti-snoring mouthpieces have given many people calmer nights without surgery or expensive and bulky machines. Most of these devices fall into two main groups:
Mandibular Advancement Devices (MADs) move the lower jaw forward a little.
Tongue Retaining Devices (TRDs) hold the tongue forward with gentle suction.
Both of these styles aim to keep the airway open so the tissues in the throat stop vibrating as you breathe. and snoring quiets down.
At Snoring HQ, we focus on giving clear, unbiased guidance instead of pushing whatever pays the highest commission. In this guide, we walk through how MADs and TRDs work, where each shines, and where each falls short.
By the end, it should be easier to match the right style of mouthpiece to dental health, jaw comfort, and breathing habits so better sleep feels like a realistic goal, not a guessing game.
As many sleep clinicians like to say, “Snoring is a symptom, not a personality trait you just have to accept.”
Key Takeaways
MAD devices hold the lower jaw slightly forward so the airway stays more open. TRD devices hold the tongue in a gentle forward grip instead. Both approaches help quiet simple snoring by stopping loose tissue from vibrating as air passes through the throat.
MAD devices are widely studied and can be molded and adjusted for a closer fit, yet they depend on healthy teeth and a stable bite. TRD devices sit outside the teeth and place no pressure on the jaw, so they suit dentures, braces, and TMJ problems better. Comfort and dental status are often the deciding factors between the two.
Both device types bring a short adjustment period with side effects such as jaw soreness for MAD users or tongue tenderness for TRD users. At Snoring HQ we compare specific products without bias, explain these trade‑offs in plain language, and help match the device style to the person rather than the other way around.
What Are Anti-Snoring Mouthpieces and How Do They Work?
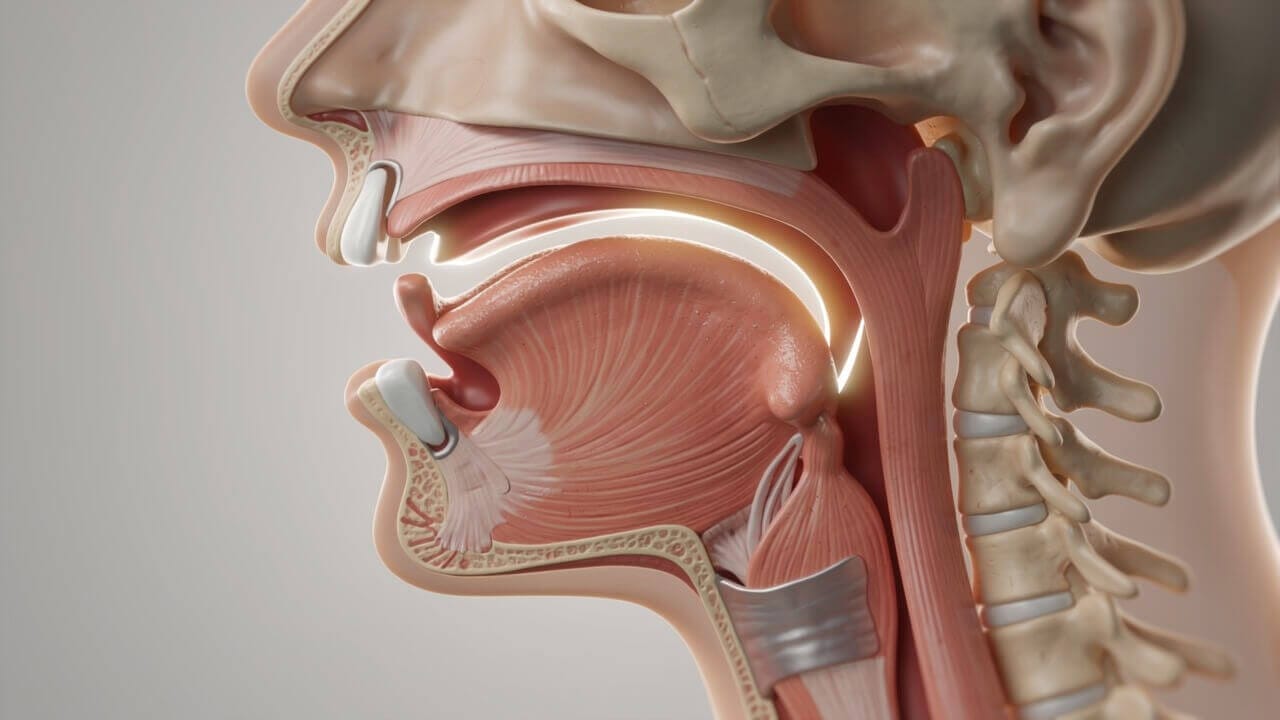
Snoring usually starts when muscles in the throat relax during sleep and the airway narrows. The tongue and soft tissue at the back of the mouth slide backward, and air has to squeeze through a smaller gap.
That narrow space makes the tissue flutter, which produces the rattling sound that keeps people awake.
Several factors raise the odds that this vibration happens, including:
Sleeping flat on the back, which lets gravity help pull the tongue toward the throat
Drinking alcohol before bed, which relaxes throat muscles more than usual
Extra weight around the neck and upper body, enlarging the tissues involved
Chronic nasal stuffiness or allergies
A naturally narrow airway or smaller jaw structure
Anti-snoring mouthpieces are small oral appliances that help keep that airway from collapsing. They do this in two main ways:
Mandibular Advancement Devices (MADs) move the lower jaw forward just a few millimeters, which also shifts the tongue and soft tissue away from the back of the throat.
Tongue Retaining Devices (TRDs) grip the tip of the tongue and hold it slightly forward so it cannot slump back and block airflow.
When the airway remains open, air flows more smoothly and the tissue does not vibrate as much. For many people with simple snoring, a well‑fitted mouthpiece brings major relief at a drastically lower cost than custom dental devices, or CPAP gear.
That said, anyone who suspects obstructive sleep apnea should talk with a doctor first, since over‑the‑counter mouthpieces are not considered a recommended way to handle that condition on their own.
Understanding Mandibular Advancement Devices (MADs)

Mandibular Advancement Devices (MADs) are the most common style of anti-snoring mouthpiece and have a strong research base behind them. They look a bit like a sports mouthguard that covers both upper and lower teeth.
When worn at night, the device holds the lower jaw a little forward, which helps keep the base of the tongue and soft tissue away from the back of the throat.
That small shift tightens the muscles along the airway and gives air more room to pass. With less crowding, tissue does not flap around as much, so snoring often quiets or stops.
For some people with mild or moderate obstructive sleep apnea, doctors even prescribe custom MADs as part of a full treatment plan.
There are two main types of MAD:
Over‑the‑counter “boil and bite” MADs
These use a thermoplastic material that softens in hot water. After heating, the user lets the device cool briefly, bites down, and presses around the edges with lips and tongue. Once the plastic sets in cold water, it holds that new shape and fits closely to the teeth.Custom prescription MADs
These come from a dentist who takes impressions or digital scans, then a lab builds a device made for that mouth only. They tend to feel most comfortable and last longer, and yet they cost far more.
Better‑quality MADs add several useful features:
Small step‑by‑step adjustability, allowing the lower tray to slide forward in one millimeter steps, so the user can start with a mild setting and move forward slowly until snoring improves
Slight side‑to‑side motion so the jaw does not feel locked in place
Small frontal breathing ports, which help people who sleep with the mouth open due to nasal blockage or habit
MADs are not right for everyone, though they help many people who snore. The match with dental and jaw health matters a lot:
Often a good match:
People with healthy teeth and gums often do well with this style. Those whose snoring is worse on their back, and people who grind their teeth (bruxism), may gain extra benefit because the device also acts as a night guard. Many partners notice quieter nights once the right advancement setting is found and used regularly.Often a poor match:
People with dentures, bridges, loose teeth, major gum disease, or known TMJ pain should avoid this style. The pressure on the teeth and jaw joint can make those problems worse over time. In those cases a dentist or sleep doctor can suggest other options that keep the airway open without stressing already sensitive areas.
Understanding Tongue Retaining Devices (TRDs)

Tongue Retaining Devices (TRDs), sometimes called tongue stabilizing devices, take a different route to the same goal. Instead of moving the jaw, they hold the tongue itself in a forward position. The device usually looks like a small soft cup or bulb that rests between the lips and teeth with a hollow in front.
Before sleep, the user:
Squeezes the bulb
Places the tip of the tongue inside
Lets go to create gentle suction
This gentle suction keeps the tongue from sliding backward during the night. With the tongue held in front of the teeth, the space behind it stays more open so air can move through the throat with less noise.
Most TRDs come in a universal fit design. There is no boiling or molding step and no need for dental impressions.
In many cases the same device works for people with natural teeth, partial dentures, full dentures, or even no teeth. A few brands offer more than one size, yet they still focus on simple shapes that do not anchor to individual teeth.
Because a TRD does not grip the teeth or shift the jaw, it places no force on the bite or the jaw joints. That single feature makes it very appealing for people with TMJ disorders, sore joints near the ears, or a history of jaw locking. It also helps anyone whose dental work rules out a MAD.
The ideal match for a TRD looks different from the typical MAD user:
Often a good match:
People who wear dentures, bridges, braces, or have unstable teeth often fit this style well. Those with TMJ pain or sensitive jaw joints also tend to prefer the lack of jaw pressure. Many who found MAD devices unbearable discover that a tongue‑based device feels more manageable once the first week passes.Often a poor match:
People who breathe through the mouth most of the night may not do well with a TRD. The device sits between the lips and can make mouth breathing hard or impossible. Some users also dislike the suction feeling on the tongue or the bulk at the front of the mouth. For them, a jaw‑based mouthpiece or another approach may feel better.
Research on TRDs is thinner than on MADs, yet many users still report strong snoring relief when they find a brand and size that matches their needs.
MAD vs. TRD: Head-to-Head Comparison

Both MADs and TRDs aim to quiet snoring by opening the airway, yet they go about it in different ways, with research comparing mandibular advancement vs combined approaches to help determine optimal treatment strategies.
The right choice depends on how someone breathes, the state of their teeth and jaw, and what feels comfortable night after night. Looking at them side by side makes these trade‑offs easier to see.
Here is a simple comparison across key features.
Feature | MAD (Jaw Advancement) | TRD (Tongue Holding) |
|---|---|---|
Main action | Moves the lower jaw forward a few millimeters so tissue tightens and the airway widens. | Creates suction on the tongue so it stays forward and cannot slump into the throat. |
Fit and adjustment | Often uses boil and bite molding plus small forward steps to fine tune snoring control and comfort. | Usually one size with no adjustment, sometimes sold in a few sizes to match tongue and lip size. |
Teeth and dental needs | Needs a set of stable, healthy teeth because the device grips the dental arches to stay in place. | Works with dentures, implants, or very few teeth since it rests on gums and lips instead of teeth. |
Jaw and TMJ impact | Can stress the jaw joint and may aggravate TMJ pain or stiffness if those problems already exist. | Keeps the jaw in a natural position and adds no pressure to joints, which people with TMJ often prefer. |
Comfort and common effects | Users often notice early jaw soreness, tooth pressure, drooling, or a dry mouth that tends to fade with regular use. | Users often feel tongue soreness, extra drooling, dry lips, or an odd bulky feeling at first that usually settles over time. |
Mouth breathing and grinding | Air holes often allow mouth breathing and the device also acts as a barrier for tooth grinding. | Can limit mouth breathing and offers no shield against grinding because the teeth still meet. |
Research and use history | Widely used for simple snoring and, with a prescription, some cases of sleep apnea. | Less research and smaller user base, yet still helpful for many people who cannot wear a jaw device. |
No chart can pick the right device for every person, yet it does highlight a pattern.
People with strong teeth, no jaw pain, and a need for adjustment often do best with a MAD. People with dentures or TMJ concerns frequently land on a TRD as a better match.
Comfort and quiet nights matter more than the label on the box, so personal testing within a trial period is often the final deciding step.
Key Factors to Consider When Choosing Between MAD and TRD

Once the basic differences between MAD and TRD make sense, the next step is to match those features to real‑life needs. That means looking closely at teeth, jaw comfort, airway habits, and even budget. No device style wins for everyone.
Key points to think about include:
Dental health matters a lot. Strong, stable teeth can usually handle the gripping force of a MAD without trouble. Loose teeth, sore gums, or a full denture plate make a TRD safer and more comfortable.
Jaw history should guide the choice as well. Anyone with TMJ pain, clicking joints, or a history of jaw locking may find a MAD hard to tolerate. TRD devices avoid forward pressure on the jaw, which often feels kinder to sensitive joints.
Breathing habits also come into play. Some people breathe mainly through the nose, while others rely on the mouth because of allergies or a blocked nose. Mouth breathers usually need a MAD with clear air holes so they do not feel short of air.
Comfort preferences differ from person to person. Some people find a firm grip on the teeth acceptable but cannot stand tongue suction. Others feel fine with a small cup on the tongue and dislike any force on the teeth or jaw.
Fine‑tuning options can help narrow the field. An adjustable MAD lets users advance the jaw step by step until snoring drops without adding too much soreness. TRD devices offer far less adjustment, so they suit those who want simple use more than detailed control.
Teeth grinding at night is another important clue. A MAD often doubles as a night guard and protects the enamel from wear. A TRD does nothing for grinding because the teeth still touch.
Money and value affect many buying decisions. Over‑the‑counter MADs with adjustable parts tend to cost toward the top of the general price range. TRDs and simpler MADs often cost less at the start yet may wear out faster with heavy use.
Trial periods can remove some risk from this process. Many brands let new users test a device for several weeks and send it back if it does not help. That window makes it easier to try the device type that seems right on paper and confirm it in the real bedroom.
Cleaning and daily care should not be ignored. Simple shapes without hinges, such as most TRDs, usually wash up faster under the tap with a toothbrush. More detailed MADs can trap debris around joints and need a bit more patience each morning.
There is no single best anti-snoring mouthpiece. The best choice is the one that fits the mouth, eases snoring, and feels comfortable enough to wear every night.
How Snoring HQ Can Help You Make the Right Choice
Sorting through dozens of brands, models, and bold claims is hard when someone is already tired and short on patience.
That is why we built Snoring HQ as an independent guide focused on sleep health instead of sales pressure. We spend our time testing devices, reading the fine print, and turning that detail into plain language.
On Snoring HQ, it is easy to find in‑depth reviews of popular MAD and TRD products along with clear comparisons that show how they differ in fit, adjustment range, and comfort. We explain which devices work better for dentures, which handle heavy grinding, and which feel slimmer in the mouth.
Our articles cover not only devices, but also snoring causes, sleep apnea warning signs, and broader habits that support better rest. The goal is simple: we want each reader to finish a review or guide feeling ready to choose and use a device with confidence rather than guesswork.
“The best device is the one you will actually wear every night,” is a common reminder from sleep professionals, and it guides how we review and compare products on Snoring HQ.
What to Expect: Side Effects and the Adjustment Period
Even the best‑fitting mouthpiece changes how the mouth and throat sit during sleep, so some early side effects are very common. Knowing what feels normal and what does not can make the first couple of weeks far less stressful.
Typical MAD side effects in the first days or weeks include:
Stiff or sore jaw on waking
Sensitive teeth or pressure on certain teeth
A bite that feels slightly “off” for a few minutes in the morning
Extra drooling or, in some people, a dry mouth
Typical early TRD side effects can include:
Tenderness at the tongue tip
A strange suction feeling on the tongue
Drooling or dry lips
Awareness of bulk at the front of the mouth
For most people the adjustment period lasts from a few nights up to two or three weeks. A slow start can help:
Wear the device for an hour or two while watching television to get used to the feel.
Then add sleep time once the mouth feels less surprised.
With an adjustable MAD, begin at the smallest advancement setting and move forward one step at a time.
Sip water through the evening and consider using dental wax on sore spots inside the cheeks.
Some signs mean it is time to pause and talk with a professional. Strong jaw pain that keeps getting worse, teeth that stay sore all day, or gums that bleed or swell are warning flags. No change in loud snoring after a fair trial also deserves attention.
If a partner still sees choking, gasping, or pauses in breathing, a doctor visit should not wait. Regular dental checkups are wise for long‑term MAD users as well, since small bite changes can creep in over time.
Important Safety Considerations and When to See a Doctor
Over‑the‑counter mouthpieces are built for simple snoring, not for self‑treatment of obstructive sleep apnea. Sleep apnea means that breathing stops or becomes very shallow many times a night. Left untreated, it raises the risk of high blood pressure, heart problems, and daytime accidents.
Warning signs that call for a medical check include:
Loud snoring paired with choking sounds during sleep
Gasping for air or long quiet pauses between breaths
Heavy daytime sleepiness despite “enough hours” of sleep
Morning headaches, dry mouth, or sore throat
Trouble concentrating, irritability, or low mood
If any of these sound familiar, a medical evaluation with a sleep study is far more important than a quick online order.
MADs can play a role in apnea care, yet that happens under the guidance of a sleep doctor and dentist. The devices used for this purpose are prescription medical devices cleared by the Food and Drug Administration. They come with closer monitoring so doctors can make sure breathing events truly improve, not just the snoring sound.
Some health issues mean a mouthpiece may not be safe at all. People with central sleep apnea, where the brain does not send steady signals to the breathing muscles, need other care.
Those with serious lung disease, severe TMJ disorders, or very fragile teeth and gums should talk with a doctor or dentist before placing any device in the mouth overnight.
The bottom line is simple. A diagnosis from a qualified professional gives a clear picture of what is happening during sleep.
With that information, it becomes much easier to decide whether a MAD, a TRD, a CPAP machine, or another option will give the safest path to quiet nights.
Beyond Mouthpieces: Complementary Approaches and Lifestyle Changes
Mouthpieces can do a lot, yet they work best as part of a wider plan for better sleep. Small changes in daily habits can make it easier for any device to quiet snoring and may even reduce the level of support needed.
Helpful habits and methods include:
Body weight affects the size of the airway. Even a modest loss of five to ten percent of body weight can shrink fatty tissue around the neck and throat. That extra space often makes snoring softer, and in some cases a device can move from nightly use to occasional backup.
Alcohol and sedative drugs relax throat muscles more than normal sleep. Drinks late in the evening often lead to louder snoring and more breathing events. Leaving a three‑ or four‑hour gap between the last drink and bedtime can make a clear difference.
Smoking irritates the lining of the nose and throat. Swollen tissue narrows the airway and raises snoring risk. People who stop smoking often notice quieter nights over time along with many other health gains.
Sleep position plays a large part for many snorers. Lying on the back lets the tongue drop toward the throat, while side sleeping keeps the airway more open. Body pillows, side‑sleeping belts, or even the classic tennis ball sewn into a shirt can train the body to roll less.
Head height changes the shape of the airway too. A wedge pillow or an adjustable base that raises the upper body a few inches can help gravity work in favor of clear breathing. This change pairs well with both MADs and TRDs.
Nasal congestion should not be ignored. Saline rinses, nasal strips, or allergy care from a doctor can improve airflow through the nose. When the nose works better, the mouth can stay closed more easily and snoring often drops.
Some people learn through a sleep study that they have moderate or severe sleep apnea. In that case, continuous positive airway pressure, or CPAP, remains the main treatment that holds the airway open all night. Mouthpieces can sometimes support comfort with CPAP but do not replace it for these cases.
Surgery sits at the far end of the treatment range. Options include trimming or stiffening soft palate tissue or moving parts of the jaw. Because surgery carries risk and recovery time, it usually comes after other methods fail or cannot be used.
Combining a well‑chosen device with healthy habits often brings the biggest long‑term change. Better sleep then supports more energy to keep those habits going.
A Few Final Points
MADs and TRDs both offer real help for simple snoring when matched with the right person. One holds the jaw forward, the other steadies the tongue, yet each shares the same aim of keeping the airway open so nights grow quieter and more restful.
The best choice rests on a few core questions. Teeth and gum health decide whether a jaw‑based device is safe.
TMJ pain often points toward a tongue device instead. Habitual mouth breathing favors a MAD with clear air holes, while a history of heavy grinding may also point in that direction.
As we noted above, no rating chart can pick the perfect device for everyone. Careful thought about health history, comfort limits, and sleep patterns makes far better guidance. An adjustment period is normal, so patience and small tweaks count as part of the process rather than signs of failure.
We at Snoring HQ are here to walk through that process with unbiased reviews and clear comparisons but, if there is any doubt about apnea or other medical issues, a visit with a doctor or sleep specialist should come first.
From there, the right device can support better sleep, better days, and calmer nights for both the person who snores and the person who shares the bed.
Better sleep does not have to be perfect; it has to be better than last week. Small steps add up.
FAQs
Can I Use an Anti-Snoring Mouthpiece if I Have Sleep Apnea?
Over‑the‑counter mouthpieces are designed for simple snoring, not for untreated sleep apnea. MAD devices can help some people with mild or moderate apnea, yet only when a doctor prescribes and monitors them.
A sleep study gives hard data on breathing pauses and oxygen levels. Trying to handle suspected apnea alone with an online device can leave serious health risks in place.
How Long Does It Take to Adjust to Wearing a MAD or TRD?
Most people need between three and seven nights before a mouthpiece feels somewhat normal. Some need two or three weeks before jaw soreness or tongue sensitivity fades to a mild level.
Extra drooling, dry mouth, or a strange bite feeling are common early on. Starting with short evening wear and then adding sleep hours can ease this period.
Will a Mouthpiece Work if I Breathe Through My Mouth?
Many MAD devices include breathing ports that let air move through the mouth while the device stays in place. That design helps people whose noses stay blocked by allergies or structural issues.
TRD devices sit between the lips and can make mouth breathing very hard. Mouth breathers usually do better with a well‑ventilated MAD and, when possible, treatment for the nasal problem.
How Do I Know if I Need a MAD or a TRD?
Healthy teeth, steady gums, and no TMJ history point toward a MAD as a good starting point since it offers more adjustment and stronger research backing. Dentures, braces, very few teeth, or ongoing jaw pain favor a TRD because it does not grip the teeth or move the jaw.
Habitual mouth breathing also leans strongly toward a MAD with air holes. We suggest using trial periods to test the type that matches your health profile and switching if results disappoint.
Can I Clean My Anti-Snoring Device in the Dishwasher?
It is best to skip the dishwasher because high heat and harsh detergents can warp or weaken the plastic or silicone. Daily cleaning with a soft toothbrush, mild soap, and warm water removes saliva and plaque safely.
Some people also use cleaning tablets made for retainers. Dedicated ultrasonic cleaners for oral devices add convenience for those who want a deeper clean.
What Should I Do if My Mouthpiece Is Not Reducing My Snoring?
First check the fit to see whether the device sits fully and evenly in the mouth. With an adjustable MAD, small steps of extra jaw advancement can make a big difference, as long as comfort remains reasonable.
Give the device a steady two‑ or three‑week trial with nightly use. If snoring stays loud, testing the other device type or visiting a doctor for a full sleep evaluation is wise because another treatment path may be needed.